Which Medical Plan is Right?
Evaluate Your Needs. Consider your prior health care usage and select plans and options that fit your lifestyle and needs.
- Do you take regular prescription medications?
- Are you anticipating surgery or non-preventive dental care?
- Did you experience a qualifying life event this year?
- Review your current plans to ensure you have the coverage you need.
Review this benefits website to learn about your new and existing plan options.
A little bit of planning will help you select the best plans, coverage levels, and financial programs for your unique situation.
Medical Plan Comparison
JOANN offers a selection of medical plans designed to fit your needs. Our medical plans are Preferred Provider Organization (PPO) and a Consumer Choice (HDHP) style plan that provide you access to one of the nation’s largest networks of quality providers. Prescription drug coverage, included in the medical plan, allows you to receive prescription drugs at reasonable costs from a network of retail pharmacies or through a convenient mail order program.
Please Note: if your spouse/domestic partner is eligible for medical coverage through their employer, they are not eligible for medical coverage through JOANN.
| Anthem Plans | PPO Ehanced Plan | PPO Value Plan | Consumer Choice Plan | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In-Network | Out-of-Network | In-Network | Out-of-Network | In-Network | Out-of-Network | |||||||
| Deductible (per person/family) | $600/person $1,200/family |
$875/person $2,625/family |
$1,500/person $3,000/family |
$3,500/person $10,500/family |
$2,000/person $4,000/family |
$4,500/person $13,500/family | ||||||
| Out-of-Pocket Maximums (per person/family) | $4,500/person $11,000/family |
Unlimited (both) | $6,350/person $12,700/family |
Unlimited (both) | $6,450/person $12,700/family |
Unlimited* | ||||||
| Covered Services (what you pay after your plan year deductible has been met) | ||||||||||||
| Physician Office Visit | $30 co-pay** | 40% | 20% | 40% | 20% | 40% | ||||||
| Specialist Office Visit | $45 co-pay** | 40% | 20% | 40% | 20% | 40% | ||||||
| Preventive Care Services*** | Covered at 100% | Not Covered | Covered at 100% | Not Covered | Covered at 100% | 40% | ||||||
| Emergency Room Visit | 20% after $250 co-pay**** | 20% after $250 co-pay**** | 20% after $250 co-pay**** | 20% after $250 co-pay**** | 20% | 20% | ||||||
| Hospital Admission | 20% | 40% | 20% | 40% | 20% | 40% | ||||||
| Retail Wellness Clinics | 20% | 40% | 20% | 40% | 20% | 40% | ||||||
| *Out-of-Network costs are not included in the out-of-pocket maximum | ||||||||||||
| **The PPO Enhanced plan office visits are not subject to deductible | ||||||||||||
| ***See preventive care section for a list of covered services in the SPD | ||||||||||||
| ****No coverage for non-emergencies, co-pay waived if admitted | ||||||||||||
Note: Please consult plan documents for full benefits, exclusions, and limitations.
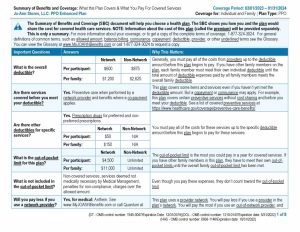
PPO Enhanced Plan SBC

PPO Value Plan SBC
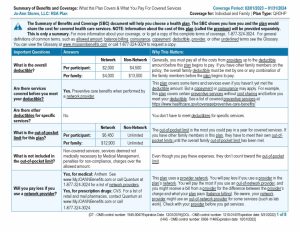
Consumer Choice Plan SBC
