Cost of Coverage
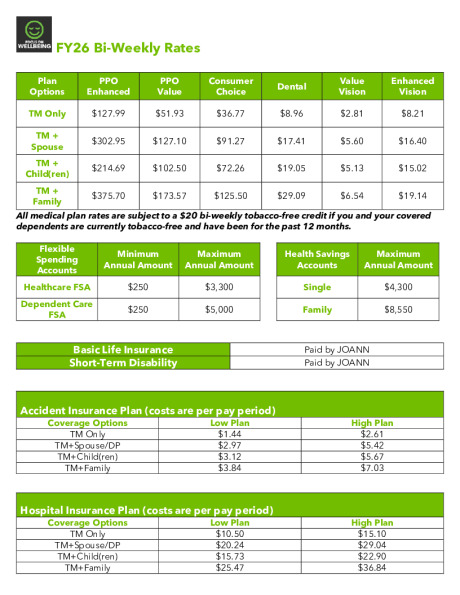
| Bi-Weekly Rates | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Plan Options | PPO Enhanced | PPO Value | Consumer Choice | Dental | Value Vision | Enhanced Vision | ||||||
| TM Only | $127.99 | $51.93 | $36.77 | $8.96 | $2.81 | $8.21 | ||||||
| TM +Spouse | $302.95 | $127.10 | $91.27 | $17.41 | $5.60 | $16.40 | ||||||
| TM +Child(ren) | $214.69 | $102.50 | $72.26 | $19.05 | $5.13 | $15.02 | ||||||
| TM +Family | $375.70 | $173.57 | $125.50 | $29.09 | $6.54 | $19.14 | ||||||
| All medical plan rates are subject to a $20 bi-weekly tobacco-free credit if you and your covered dependents are currently tobacco-free and have been for the past 12 months. | ||||||||||||
| Domestic Partner Rates | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All Rates Bi-weekly | TM + DP | TM + TM Child(ren) & DP |
TM + DP & DP Child(ren) |
TM + TM Child(ren) & DP & DP Child(ren) | ||||||
| PPO Enhanced | Pre-Tax | $127.99 | $214.69 | $127.99 | $214.69 | |||||
| PPO Enhanced | Post Tax | $174.96 | $161.01 | $247.71 | $161.01 | |||||
| PPO Enhanced | Imputed Income | $680.28 | $808.66 | $895.36 | $808.66 | |||||
| PPO Value | Pre-Tax | $51.93 | $71.07 | $51.93 | $102.50 | |||||
| PPO Value | Post Tax | $75.17 | $65.45 | $121.64 | $71.07 | |||||
| PPO Value | Imputed Income | $684.95 | $830.47 | $881.04 | $830.47 | |||||
| Consumer Choice | Pre-Tax | $36.77 | $72.26 | $36.77 | $72.26 | |||||
| Consumer Choice | Post Tax | $54.50 | $53.24 | $88.73 | $53.24 | |||||
| Consumer Choice | Imputed Income | $665.68 | $817.12 | $852.61 | $817.12 | |||||
| Dental | Pre-Tax | $8.96 | $19.05 | $8.96 | $19.05 | |||||
| Dental | Post Tax | $8.45 | $10.04 | $20.13 | $10.04 | |||||
| Dental | Imputed Income | $17.82 | $25.70 | $23.97 | $25.70 | |||||
| Value Vision | Pre-Tax | $2.81 | $5.13 | $2.81 | $5.13 | |||||
| Value Vision | Post Tax | $2.79 | $1.41 | $3.73 | $1.41 | |||||
| Enhanced Vision | Pre-Tax | $8.21 | $15.02 | $8.21 | $15.02 | |||||
| Enhanced Vision | Post Tax | $8.19 | $4.12 | $10.93 | $4.12 | |||||